Powered By



 Continue with Facebook
Sign up with your email
Continue with Facebook
Sign up with your email
Epilepsy treatments — including surgical interventions — have become more advanced and effective in the past decade. Some people living with epilepsy reach a point in their treatment when they may become good candidates for neurosurgery. This is especially the case for people who are taking multiple anti-seizure medications and still experiencing breakthrough seizures. This is known as medically refractory epilepsy.
One MyEpilepsyTeam member said, “I’ve been through four different medications and still do not have control over the seizures. Every neurologist I have seen tells me I need brain surgery.”
In recent years, epilepsy surgery has quickly evolved to be less invasive, with fewer side effects and better outcomes. The goal of surgery is to reduce the frequency of seizures and improve quality of life for people with drug-resistant epilepsy. Three types of epilepsy surgery include:
All people with epilepsy deserve to know about the latest available treatments for seizure control. This article will review different minimally invasive surgery options, their risks and benefits, and how to know if you are a good candidate for surgery.
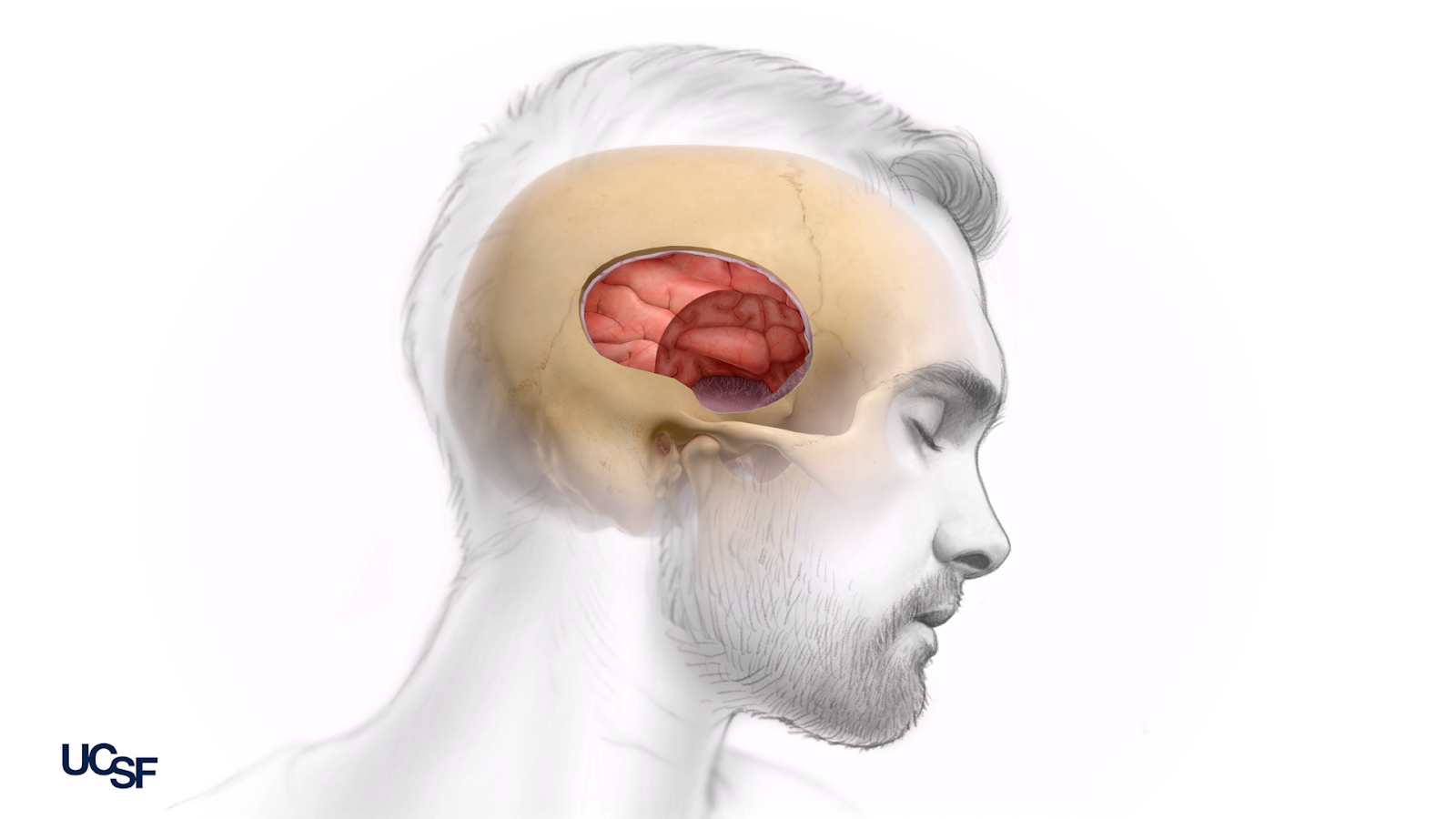
Craniotomy is the oldest, and most invasive, form of epilepsy surgery. The goal of craniotomy is to remove part of the brain that causes seizures, also known as the seizure focus. This requires an open surgery under general anesthesia. Good candidates for craniotomy have seizures that originate in one specific area of the brain. The closer this region is to the outside of the brain (the cortex), the easier it is to surgically remove and the more likely a neurosurgeon will offer craniotomy as a treatment option.
After the incision is closed, people generally stay in the hospital for three to five days. Depending on where the craniotomy was performed in the brain, people may have postsurgical speech and memory symptoms. These often improve over time.
A collection of six systematic reviews (high-quality research studies that combine the results of several studies) found between 43 percent and 75 percent of people reported being seizure-free after craniotomy.
One MyEpilepsyTeam member described their quick recovery from a craniotomy. “I am a physical therapist and I was back to work, lifting patients, six weeks post-op.” Another discussed a decrease in epilepsy symptoms months after their craniotomy: “Luckily, I am now seizure-free for four months. Before, I had seizures every night.”
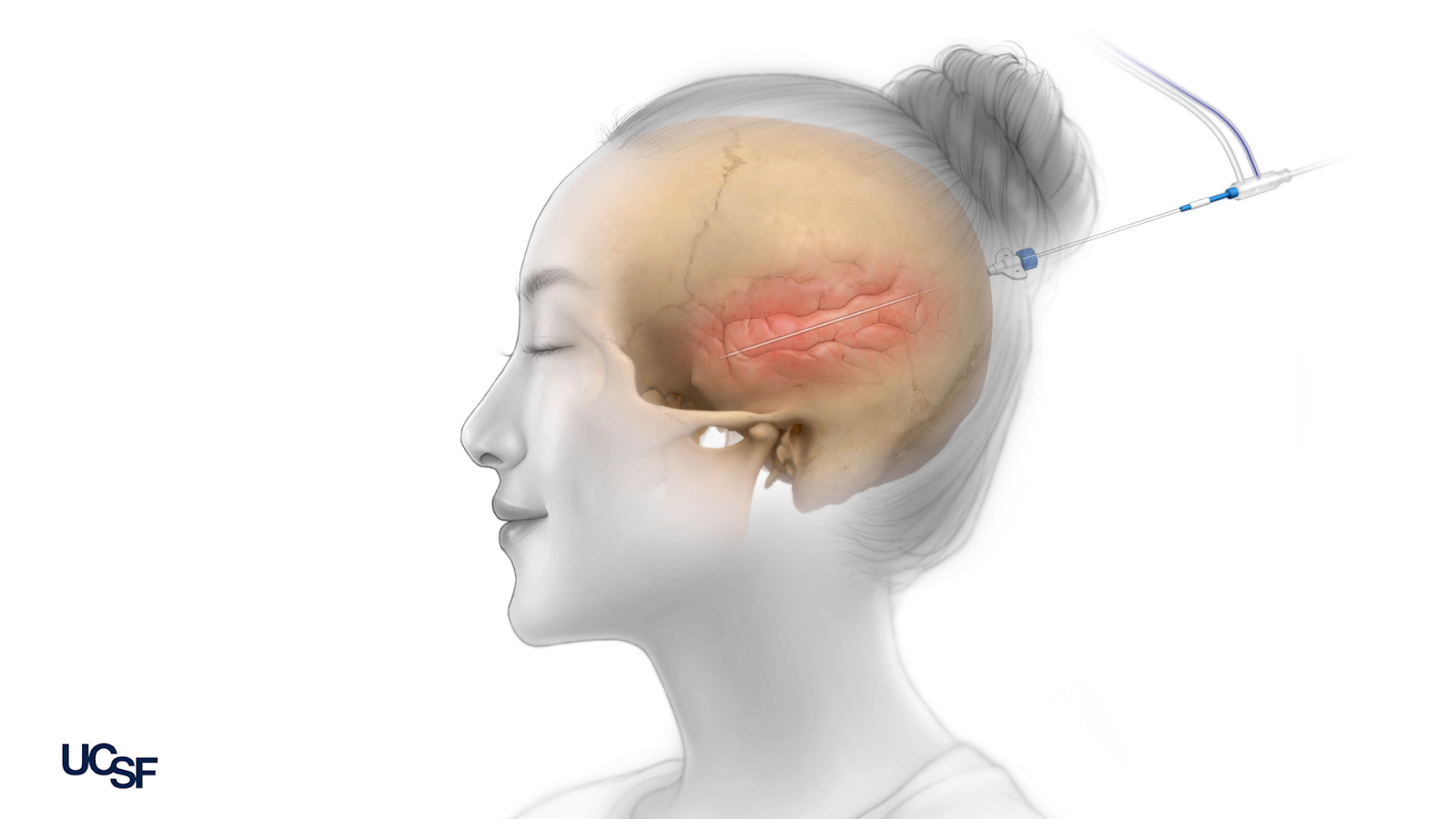
Laser interstitial thermal therapy (LITT), also called ablation, is a modern surgical technique that is considered a minimally invasive procedure — especially when compared to a craniotomy. To be eligible for laser ablation surgery, your seizures must originate from one specific part of your brain. Many people who receive ablation have mesial temporal lobe epilepsy, which happens in a region of the brain that is easier to access with the ablation technique.
Although ablation is considered less invasive, it still requires you to go under general anesthesia and have an incision. During ablation, a long, thin metal device is inserted into the scalp and skull to reach the part of the brain that contains the seizure origin point. The incision is about the width of a pencil tip.
Once the device has reached the affected brain tissue, neurosurgeons carefully heat the tip of the device. This burns and destroys the region causing seizures without damaging the surrounding areas of the brain. By destroying this focal area, the hope is to reduce the frequency of seizures. During this procedure, doctors use MRI as well as a computer program to ensure pinpoint accuracy. After the procedure, the small incision is closed.
In one review that combined results from 13 different studies, the overall seizure freedom rate for people who’d had LITT was 58 percent. About 17 percent of people had some complication from the surgery. A typical hospital stay for ablation is one to two days, and most people return to normal functioning within a week.
As opposed to removing or targeting the parts of the brain causing seizures in people with epilepsy, minimally invasive neuromodulation surgeries use electric stimulation in carefully controlled ways to predict and stop seizures in real time. There are three ways surgeons currently perform this minimally invasive brain surgery: through responsive neurostimulation (RNS), deep brain stimulation (DBS), and vagus nerve stimulation (VNS). Eligibility for each of these surgical options varies, based on where seizures originate in your brain.
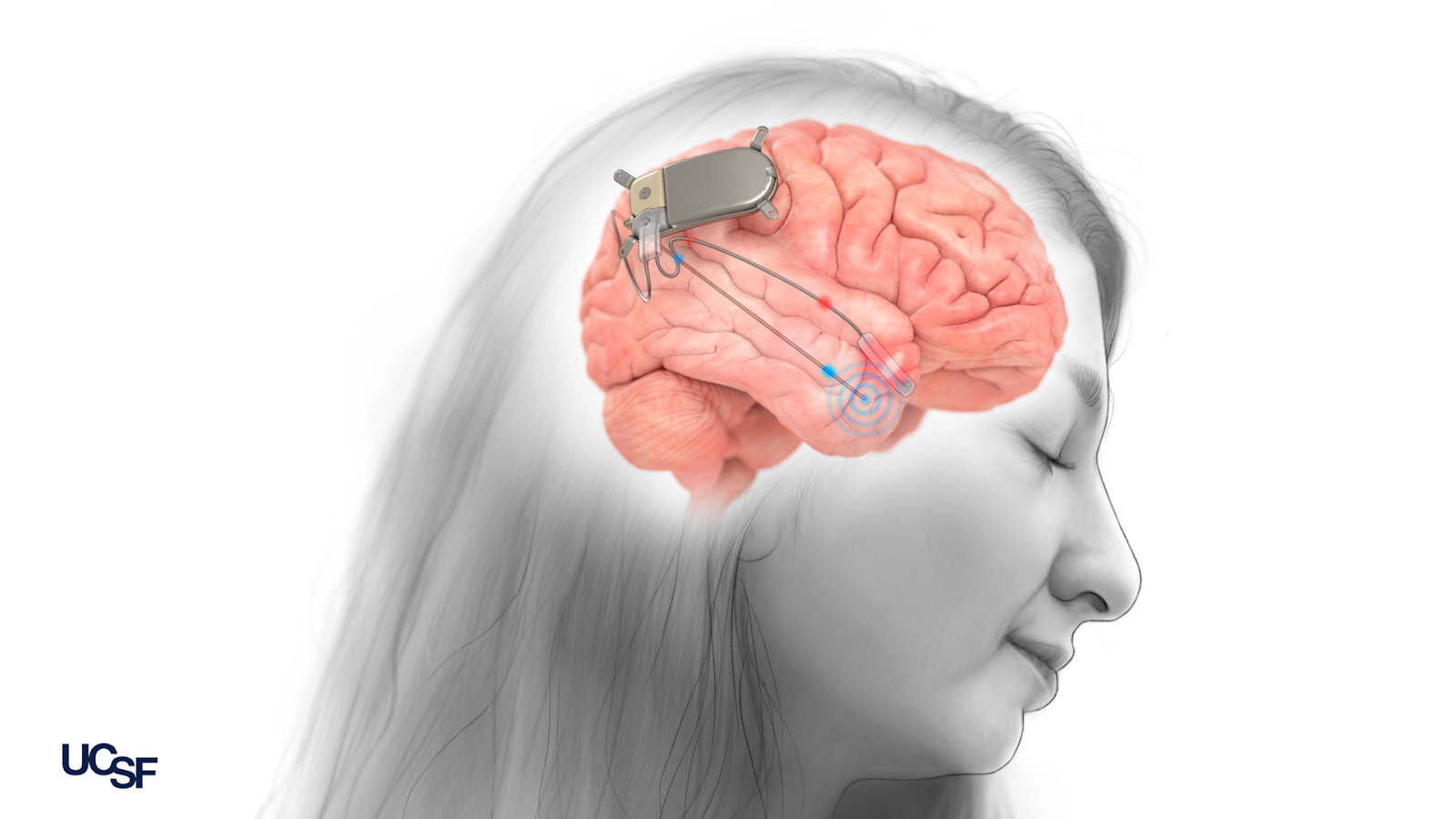
One neuromodulation option is called responsive neurostimulation, which includes an electrode (a piece of metal that carries electricity) inserted in or on the part of the brain causing seizures. This system also includes a device that can record seizure activity and deliver stimulation to the brain to stop and prevent seizures. The effectiveness of RNS improves over time because the settings can be adjusted carefully by doctors, based on your brain’s patterns.
One study published in the journal Neurology examined RNS in 230 participants over the course of nine years. Most people reported having less seizures after RNS. About 18 percent of participants went more than a year without a seizure, and many of this group were seizure-free for three years.
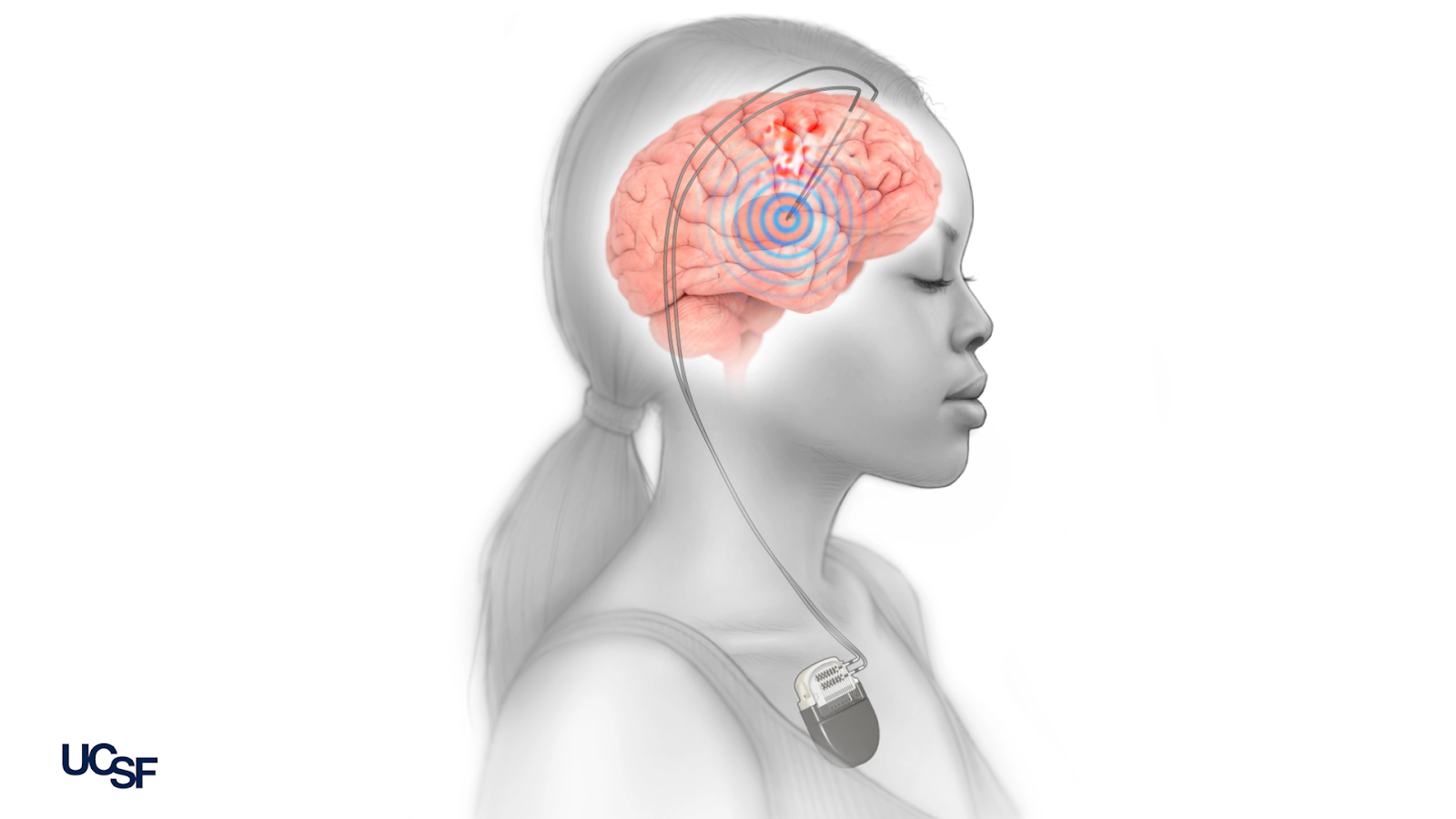
The second kind of neuromodulation is called deep brain stimulation. In DBS, an electrode is implanted into the affected part of the brain and a stimulating device is placed under the skin of the chest. The surgeon placing the brain electrode is carefully guided with MRI. The chest device is like a pacemaker for the brain, sending electrical signals to the brain electrode to prevent and stop seizures.
DBS was approved by the U.S. Food and Drug Administration (FDA) in 2018. One review of several studies, published in the journal Epilepsia, showed that over half of people experience a 46 percent to 90 percent seizure reduction when DBS targets a part of the brain called the thalamus. DBS has a slightly higher effectiveness when it targets the hippocampus region of the brain.
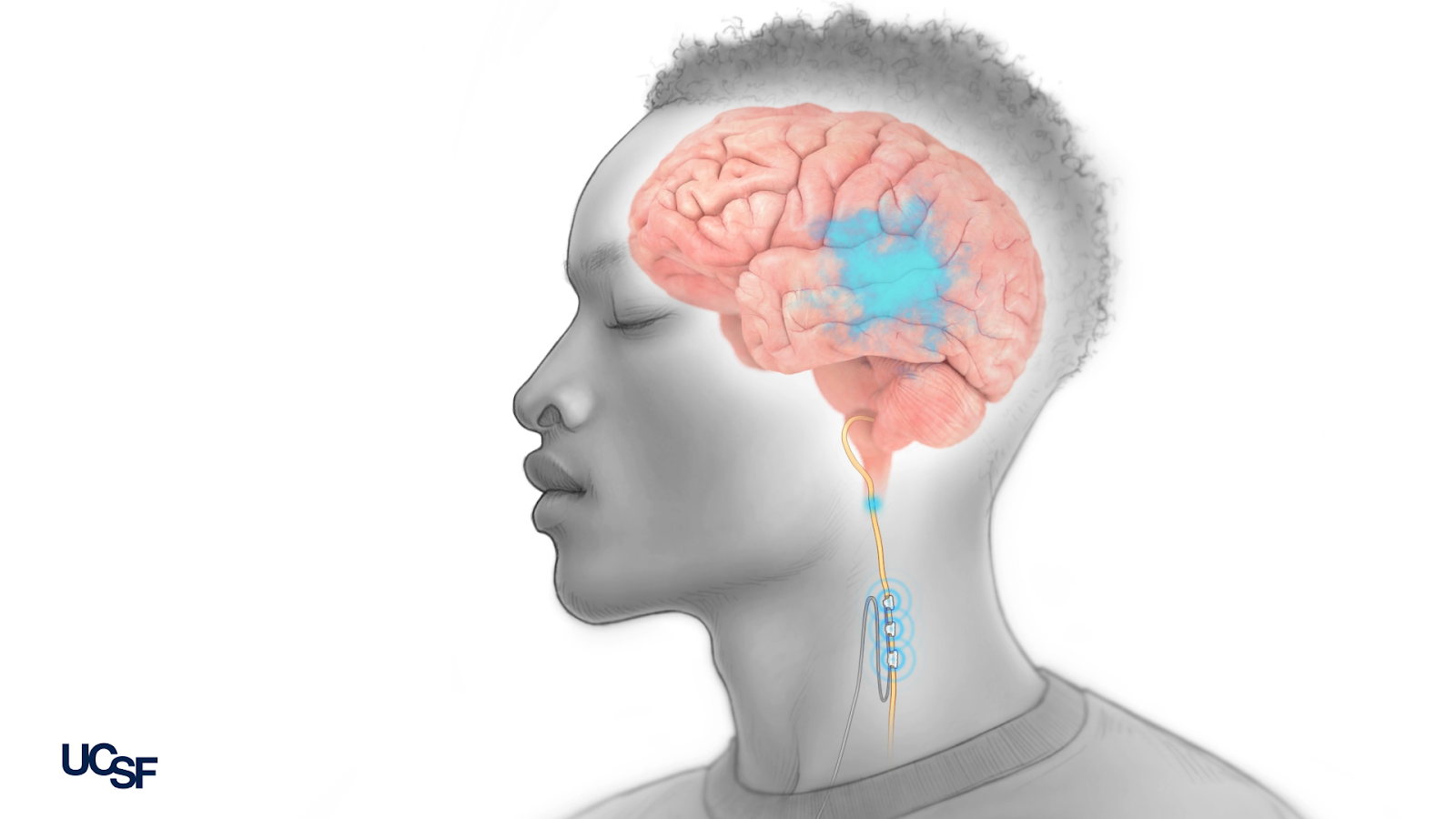
One final minimally invasive option is vagus nerve stimulation. The vagus nerve runs through your neck and sends signals between your brain and body. In VNS, surgeons insert a small electrical device under the skin of your chest that is then attached to the vagus nerve in the neck. This device sends electrical signals to the vagus nerve on a regular schedule, which has been shown to prevent seizures from occurring over time. People may be eligible for VNS when brain surgery is not possible or has not worked. VNS can work for people who may have multiple seizure sites of origin in their brain.
While VNS is less invasive than other forms of surgery, it is also less effective. One collection of studies estimated that seizure frequency after VNS insertion was reduced by about 45 percent. Certain types of epilepsy have a higher rate of successful treatment with VNS. However, VNS rarely leads to complete seizure freedom, and approximately 25 percent of people who have the procedure will not see any improvement.
One MyEpilepsyTeam member described their experiences with VNS: “Since my VNS was inserted 12 years ago (with one battery change two years ago), my seizures have been controlled. I have a checkup every six months.”
Medical and surgical treatment options for epilepsy are evolving quickly, and it can be hard to stay informed on all of your options. Neuromodulation, craniotomy, and ablation are all different surgical techniques to improve quality of life with epilepsy. It is likely you would continue to take medications after surgery. Each surgical treatment has different risks and benefits that are important to research and discuss with your doctor.
Surgery only works for a subset of people with epilepsy, and each type of surgery has different criteria for eligibility. You have the power to discuss with your neurologist and neurosurgeon which options, if any, will work best for you. Talk to your doctor about all of your options for epilepsy treatment, including the latest advancements in medication and surgery.
Watch a video about minimally invasive epilepsy surgery on UCSF's Youtube channel here.
MyEpilepsyTeam is the social support network for people with epilepsy and their loved ones. On MyEpilepsyTeam, more than 111,000 members come together to ask questions, give advice, and share their stories with others who understand life with epilepsy.
Has surgery been part of your treatment for epilepsy? If not, have you ever discussed brain surgery for epilepsy with your doctor? Share your experiences and thoughts in the comments below or by posting on MyEpilepsyTeam.
Get updates directly to your inbox.



My Brain Surgery Was 3/07/1991, I Believe It Was Called A 'Lobectomy??'


 Continue with Facebook
Sign up with your email
Continue with Facebook
Sign up with your email
Become a member to get even more





 Join
Join


A MyEpilepsyTeam Member
Last summer my husband started experiencing more seizures, developed balance issues and lost his sense of taste/scent. His meds were at a high dose and were the plausible cause of some symptoms… read more
We'd love to hear from you! Please share your name and email to post and read comments.
You'll also get the latest articles directly to your inbox.